Feel the squeeze: groin strain risks and prevention

Groin strain is one of leading causes of injury in sports involving running and jumping. Sports Performance Bulletin outlines the risk factors for injury and provides injury prevention strategies
Groin injuries and the pain they produce can be a frustrating problem for athletes, especially those whose sports involve sprinting and/or rapid accelerations and decelerations. The exact incidence of groin injury in most sports is unknown because athletes can often play through minor groin pain and the injury goes unreported. In addition, overlapping diagnoses can skew the incidence. However, studies in this area generally suggest that groin injury accounts for between 2-5% of all sports injury(1). Of these, the most prevalent groin injury in sport is the adductor strain, which for example in soccer players, accounts for an incidence rate of around 10% - 18% of groin strains(2,3).Injury diagnosis
The groin and hip region is made up of a number of different structures that interact with each other (see figure 1). These include the pubic bones and symphysis, musculature, tendons, aponeuroses, ligaments, the inguinal canal, hip joint etc. Consequently athletes often report a pain or pain pattern that cannot be uniquely assigned to a single structure. In addition, there are a multitude of various nerves in the groin region responsible for providing sensation, and which support movement. Any compression of these nerves (known as ‘entrapment syndrome’) can lead to significant stress-related pain(4,5).Figure 1: simplified diagram of groin anatomy
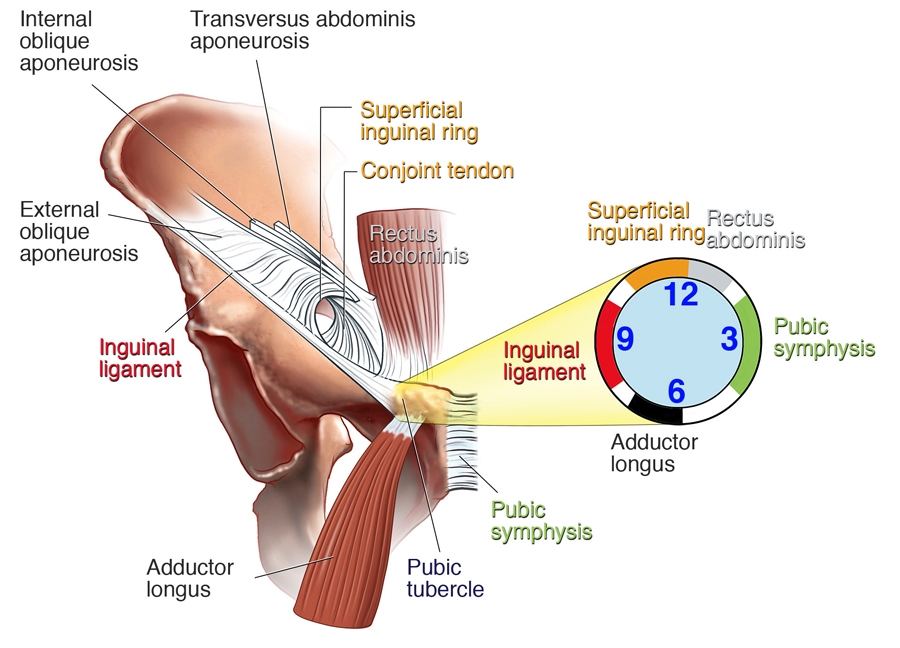
NB: The ‘clock’ shows the approximate insertion locations of the inguinal ligament, adductor longus, pubic symphysis, rectus abdominis and the superficial inguinal ring.
Diagnosis of a groin strain requires a detailed clinical investigation by a clinician with good knowledge of the (complex) anatomy of the groin and pelvic region, and an understanding of the interaction of affected structures. In addition to a clinical examination, imaging (eg X-ray, MRI etc) may also be required to make a definitive diagnosis. This is especially the case given that typical groin pain symptoms can have causes other than a groin strain. Table 1 provides a summary of possible other causes (differential diagnoses), highlighting the difficulty in making an accurate diagnosis(6-8).
Table 1: Other (non-strain) causes of groin pain in competitive athletes(8) |
| ACUTE ONSET |
| · Fascicle rupture etc.) |
| · Avulsion and apophyseal injury |
| · Fracture |
| GRADUAL ONSET |
| · Osteitis pubis, symphysitis |
| · Weak groin, inguinal hernia |
| · Pathology of the hip joint (labral lesions) |
| · Femoroacetabular impingement (FAI)) |
| · Snapping hip |
| SPINAL COLUMN DISORDERS |
| · Disc prolapse with nerve root inflammation |
| · Blockage in the lumbar spine region |
| · Spondylolisthesis |
| FUNCTIONAL IMPAIRMENT OF THE PELVIS |
| · Blockage of the iliosacral joints |
| · Pelvic torsion |
Despite the large number of possible differential diagnoses, groin strains involving muscular injuries of the adductors (inner thigh muscles), the iliopsoas muscle and abdominal musculature are the most frequent causes of acute groin pain in sportsmen and women. For example, a 2009 study looked at groin strain in elite European footballers who were playing for 23 of the top UEFA teams(9). Out of the 628 cases of groin strain, 399 (63.5%) resulted from adductor injuries, while injury to the iliopsoas muscle accounted for 52 (8.2%) cases – a combined total of nearly 72% of the reported groin injuries.
Are you at risk?
On the basis that ‘an ounce of prevention is worth a pound of cure’, understanding the risk factors that predispose an athlete to groin injury (and then reducing them) is important. In a 2013 study, researchers identified several intrinsic and extrinsic risk factors(see table 2)(10).It follows that a strength and conditioning program that addresses these factors can help prevent groin injury – or in a rehab program to speed recovery from an existing injury – something we’ll return to shortly.Table 2: Contributing Factors to the Development of Groin Pain
Extrinsic Factors Intrinsic FactorsPost-injury inadequate rehabilitation Muscle weakness
Fatigue Inadequate muscle conditioning
Decreased fitness Poor groin flexibility
Muscle tightness Poor pelvic and core stability
Inadequate warm up Increasing age
Poor posture
Neural tightness
Recurrent injury
There’s certainly solid evidence in the literature showing an association between strength or flexibility and musculoskeletal strains in various athletic populations. For example, in a study into soccer players, researchers found decreased pre-season hip abduction range of motion in players who subsequently sustained groin strains, compared with uninjured players(11).
In professional ice hockey players, adductor muscle strength has been associated with a subsequent muscle strain. For example, US researchers found that pre-season hip adduction strength was 18% lower in NHL players who subsequently sustained groin strains, compared with the uninjured players(12). The hip adduction:abduction strength ratio was also significantly different between the 2 groups; in the players who sustained a groin strain, pre-season adduction:abduction strength ratio was lower on the side that subsequently sustained a groin strain (as compared with the uninjured side). Adduction strength was 86% of abduction strength on the uninjured side but only 70% of abduction strength on the injured side.
Another study on adductor strains in ice hockey players showed that players who practiced during the off-season were less likely to sustain a groin injury(13). In this study, an additional risk factor was the presence of a previous adductor strain – consistent with a study into Australian Rules football players, where researchers reported a 32% re-injury rate(14).
In a 2007 study, researchers conducted a systemic review of the literature for risk factors in groin injury(15). They concluded that there was support for an association of previous injury and greater abductor to adductor strength ratios as well as lack of sport specificity of training and pre-season sport-specific training, as individual risk factors in groin strain injury in athletes. They also stated that core muscle weakness or delayed onset of transversus abdominal (one of the key core muscles) recruitment may increase the risk of groin strain injury. However, when it came to absolute levels of adductor strength and length, as well as age and/or sport experience, the evidence to support a causal association was only weak.
Another review study evaluated the evidence for groin injury risk factors across a wide ranges of sports(16). The researchers identified 2521 potentially relevant studies, of which 29 were included and scored. The researchers concluded that the following factors were associated with groin injury: a previous groin injury, more elite levels of play, reduced hip adductor strength (absolute and relative to the hip abductors), and lower levels of sport-specific training.
Prevention
As we saw in table 2 above, researchers have identified a number of extrinsic and intrinsic factors in the development of groin pain. It follows therefore that any prevention program should try to address one or more of these factors. And given that the adductor musculature is complex (see figure 2) and that adductor muscle injury accounts for a significant proportion of groin injuries overall, the obvious question is whether adductor strength training can help?Figure 2: Adductor muscle complex*
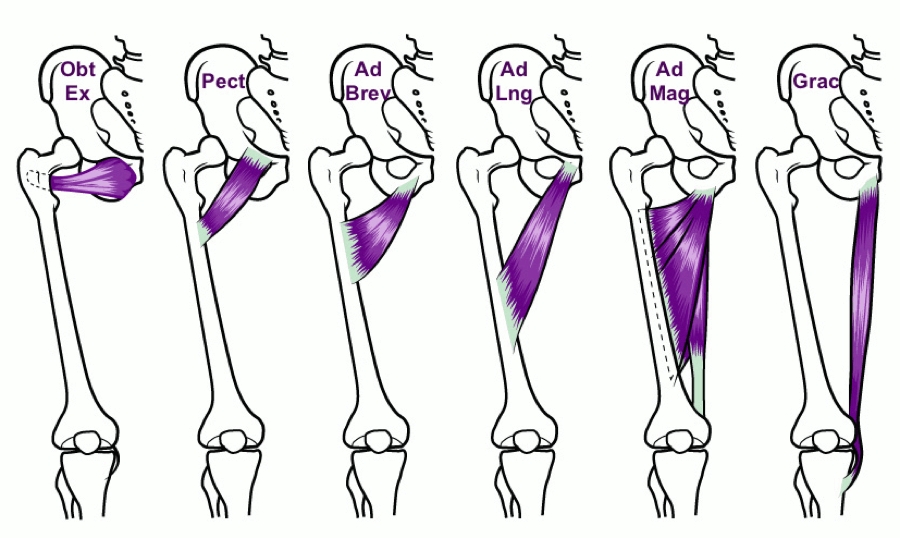
*Image provided by ChiroUp.com (www.chiroup.com). Obt Ex – obturator externus; Pect = pectineus; Ad Brev = adductor brevus; Ad Long = adductor longus; Ad Mag = adductor magnus; Grac = gracilis.
One study on strength training to prevent adductor strains in professional ice hockey players produced positive results(17). Before the 2000 and 2001 seasons, professional players were strength tested. Thirty three of the 58 players were classified as at risk, with an adduction:abduction strength ratio of less than 0.8 and were placed on an intervention program consisting of strengthening and functional exercises aimed at increasing adductor strength. Injuries were tracked over the course of the two seasons. The results showed that injury incidence was 0.71 adductor strains per 1000 player-game exposures (approximately 2% of all injuries). This compared with a pre-intervention injury rate of 3.2 per 1000 player-game exposures (approximately 8% of all injuries – four times higher).
In soccer players meanwhile, researchers showed that a generalized conditioning program was suitable for injury prevention in young male players of varied skill levels(18). The program was made up of ten exercises to improve endurance, reaction time, coordination, lower extremity stability, plus flexibility and strength of the trunk, hip, and lower extremities. In addition to nearly 50% fewer mild injuries, 41% fewer overuse injuries and 55% fewer training injuries, this program resulted in no less than 80% fewer groin injuries over the course of an entire year!
More evidence for the benefits of strength training to reduce groin strains prevalence comes from a 1999 study on athletes(19). It found that 8-12 weeks of an active strengthening program proved effective in treating chronic groin strains. The program consisted of progressive resistive adduction and abduction exercises, balance training, abdominal strengthening, and skating movements on a slide board. By contrast, a passive physical therapy program of massage, stretching was ineffective.
What kind of program?
An example of the kind of conditioning program that can help groin strain prevention in athletes is shown in table 3(20). The example given is for ice hockey players but can be adapted (in the sports-specific conditioning phase) for other sports too. Other studies also provide good evidence that this approach to rehabilitation and prevention produces positive results(21,22).Table 3: Example of adductor strain injury prevention program(20)
Warm-up
- Bike
- Adductor muscle stretching
- Sumo squats
- Side lunges
- Kneeling pelvic tilts
Strengthening program
- Ball squeezes pressing with inner thigh (legs bent and legs straight – use different ball sizes
- Concentric adduction (bringing legs together) with weight against gravity
- Adduction in standing on cable column or elastic resistance
- Seated adduction machine
- Standing with involved foot on sliding board, moving in saggital (forwards/backwards) plane
- Bilateral adduction on sliding board moving in frontal (side-to-side) plane (ie, simultaneous bilateral adduction bringing both legs to centreline of the body simultaneously)
- Unilateral lunges with reciprocal arm movements
Sports-specific training for ice hockey (should be adapted according to sport)
- On ice, kneeling adductor pulling together of legs
- Standing resisted stride lengths on cable column to simulate skating
- Slide skating
- Cable column crossover pulls using ankles
- Clinical goal - adduction strength to reach at least 80% of the abduction strength
Another great exercise for adductor strength is the ‘Copenhagen adduction exercise’, which has been shown in research to be particularly effective in soccer players(23). You can see this exercise being performed by clicking on the link below:
The Copenhagen adduction exercise
In summary
Groin injuries in athletes span a wide range of conditions, and are a major cause of missed time from sport. To make matters worse, once a groin injury has occurred, an athlete is at increased risk from a future groin injury. The good news is that many common groin injuries – particularly involving the adductor muscles - respond well to strength and conditioning programs, both as part of a post-injury rehab program and in terms of prevention. These programs start with rest and passive treatment, immediately followed by an active training program emphasizing eccentric resistive exercises.References
- Am Fam Physician. 2001;64(8):1405–14
- Int J Sports Med. 1983;4(2):124–8
- Sport Med. 2002;32(5):339–44
- Dtsch Z Sportmed 2010; 61: 33–39
- Radiographics 2008; 28: 1415–1438
- Orthopäde 2007; 36: 414–422
- Eur J Radiol 2012; 81: 3780–3792
- Radiology 2008; 247: 797–807
- Br J Sports Med 2009; 43: 1036–1340
- ‘Recurrent hamstring muscle injury: applying the limited evidence in the professional football setting with a seven-point programme’ Br J Sports Med. 2013
- Int J Sports Med. 1983;4(2):124-128
- Am J Sports Med. 2001;29(2):124-128
- Med Sci Sports Exerc. 2001;33(9):1423-1433
- Med J Aust. 1993;159(5):298-301
- Sports Med. 2007;37(10):881-94
- Br J Sports Med. 2015 Apr 1. pii: bjsports-2014-094287
- Am J Sports Med. 2002;30(5):680-683
- Am J Sports Med. 2002;30:652–6
- Lancet. 1999;353(9151):339-443
- Sports Health. 2010 May; 2(3): 231–236
- Curr Sports Med Rep. 2002;1(5):301-305
- Am J Sports Med. 2001;29(4):521-533
- Scand J Med Sci Sports. 2016 Nov;26(11):1334-1342
You need to be logged in to continue reading.
Please register for limited access or take a 30-day risk-free trial of Sports Performance Bulletin to experience the full benefits of a subscription. TAKE A RISK-FREE TRIAL
TAKE A RISK-FREE TRIAL

Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.