You are viewing 1 of your 1 free articles. For unlimited access take a risk-free trial
Femoral neck stress fracture: why groin pain should never be ignored
Femoral neck stress fracture is a serious and debilitating hip injury that can affect (especially female) runners. SPB explains how it is diagnosed & treated, and how an appropriate diet can reduce the risk of this injury

First reported by Asalin, a German military surgeon in 1905(1), a femoral neck stress fracture (which we will abbreviate as ‘FNSF’ from this point on) is a fairly uncommon but potentially very serious injury. Estimates vary, but in healthy young subjects suffering a stress fracture, FNSFs account for between 1% and 7.2% of such injuries(2). Like all stress fractures, most FNSFs in athletes are fatigue-induced fractures, which are caused by repetitive loading of normal bone with unsustainable (for the athlete in question) forces(3). However, what makes this type of injury particularly serious is that, unlike many other stress fractures, FNSFs are very often not amenable to conservative ‘rest and rehabilitation’ management techniques. This means many will require surgery, especially those that are not diagnosed early (more on this later).
What is a femoral neck stress fracture?
A femoral neck stress fracture is a fracture to the narrow ‘neck’ between the top of the femur bone and the ‘ball’ of the femur (more technically known as the femoral head), which inserts into the hip joint socket - see figure 1. Due to the anatomy and biomechanics of the main thigh bone (the femur) during activities such as running, FHSFs are usually classified according to the location of the fracture origin and the severity/progression.
Figure 1: Anatomy of the femoral neck
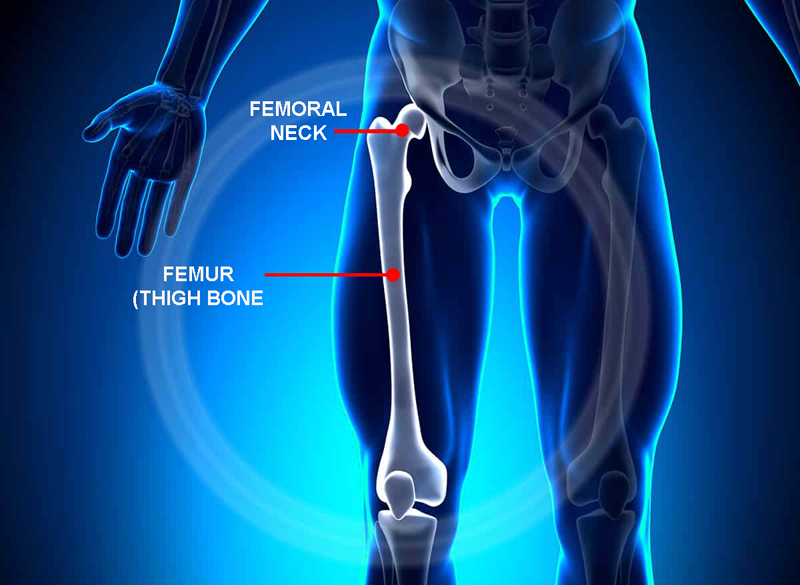
The femoral neck lies between the main bone mass of the femur and the femoral head, which inserts into the hip socket.
The neck of the femur can be thought of as a lever, through which forces generated by the muscles of the thigh and pelvis can be transmitted to the trunk (via the hip), enabling motion. Due to its profile and orientation, the femoral neck is subject to considerable compressive (squashing) and tensile (pulling) forces during activities such as running. The way these forces act upon the femoral neck can be visualized as shown in figure 2. In most cases, stress fracture resulting from tensile forces leads to a ‘tension fracture’, with the origin of the fracture on the upper side of the neck. By contrast, fracture resulting from compressive forces tends to occur on the lower side of the neck.
Figure 2: FNSF location and compressive/tensile forces
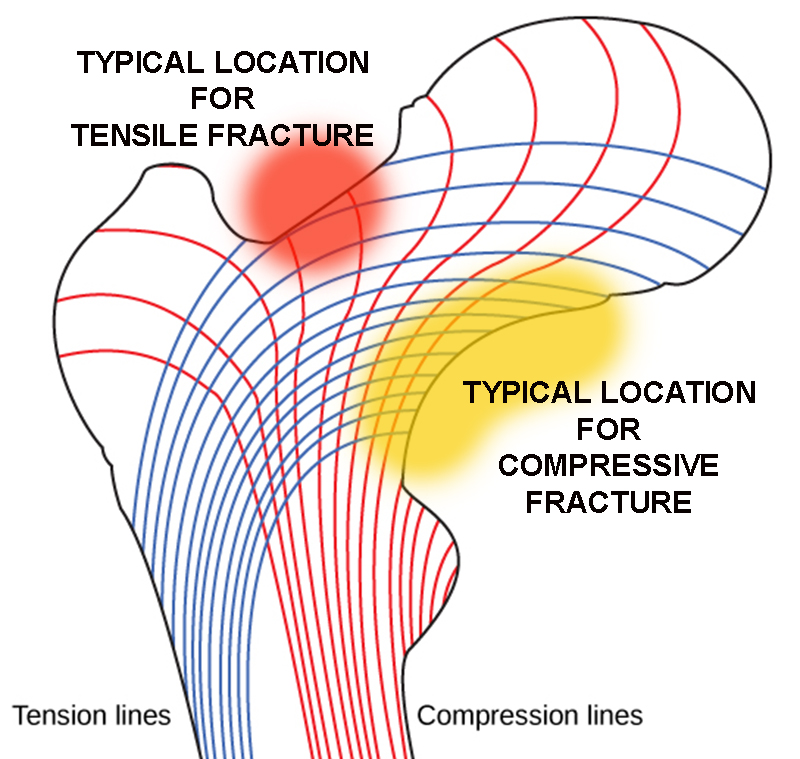
Tension = blue lines; compression = red lines. Fracture risk is increased where force line run parallel for the neck surface.
Fracture classification
There are a number of different classification systems for FNSFs. One of the earliest classification systems described is the ‘Garden classification of subcapital femoral neck fractures’, which classifies femoral neck fractures into four types - as a function of displacement – see figure 3(4). This system however was developed in the era where computer tomography (CT) and MRI imaging were unavailable, and has since shown to have limitations. In particular, many femoral neck fractures that are classified as ‘Type I’ when viewed on a simple X-ray may potentially be Garden Type II or III fractures when examined using more detailed and accurate CT or MRI imaging. Despite these limitations however, the classification is still well accepted and widely used by orthopaedic surgeons(5).
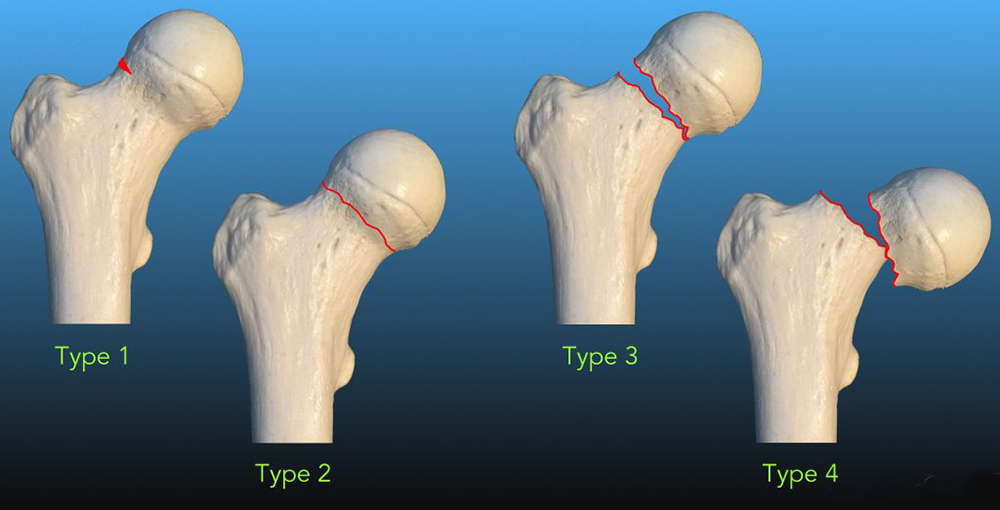
*Garden stage I: undisplaced incomplete; *Garden stage II: undisplaced complete; *Garden stage III: complete fracture, incompletely displaced; *Garden stage IV: complete fracture, completely displaced.
In general, stage I and II are stable fractures and can be treated with internal fixation (surgically pinning the head back into place thus preserving the femoral head. Stage III and VI fractures on the other hand are deemed as ‘unstable’ fractures, and hence treated by a complete hip replacement.
Currently, one of the most commonly used classifications of fracture type and severity is the ‘Fullerton and Snowdy’ classification(6). This classifies fractures into one of three categories (based on X-rays and bone scans):
- Type I – originating on the tension-side of the femoral neck.
- Type II – originating on the compression side of the neck.
- Type III – displaced fractures.
The researchers who developed this classification (Fullerton and Snowdy unsurprisingly!) concluded that fractures resulting from tension on the upper side of the femoral neck actually present a higher risk than compression fractures because they are inherently more unstable and prone to displacement. By contrast, they suggested that femoral neck fractures resulting from compressive forces on the lower side of the neck present a lower risk. This means that (depending on the extent of the fracture) they can be treated by non-surgical, conservative treatment/rehab methods (more later).
Why do femoral neck stress fractures occur?
Most athletes are able to enjoy a lifetime of training and competition without suffering a FNSF. So why is it that some athletes succumb while most don’t? Although there is a general perception that stress fracture affects male and female athletes equally, more recent research suggests that due to physiological and biochemical differences, female athletes are indeed more vulnerable. Specifically, FNSF injury is known to be more common in young female (rather than male) runners, endurance athletes and military recruits (as opposed to their male contemporaries)(7).
Underlying the cause of all FNSF injuries is the repeated loading of the femoral neck, which over a period of time, exceeds the body’s ability to adequately remodel and rebuild the affected bone tissue (where old/damaged bone is resorbed and replaced with new bone). The end result is a weakened area of bone in the femoral neck, which is vulnerable to fracture. It follows therefore that any nutritional factors that might impede efficient bone remodeling will, over time, lead to an increased FNSF risk(8). The good news is that in recent years, research has identified the following dietary/lifestyle risk factors associated with an increased FNSF risk in athletes, especially female athletes. These are as follows:
- Limited calorie intake, dairy-free and/or low-fat diets and/or eating disorders during adolescence(9,10).
- Amenorrhea (cessation of monthly periods), which leads to a 2-4 times higher risk of FNSFs compared athletes who continue to menstruate normally)(11).
- A low vitamin D status(12).
- Reduced bone mineral density in the femur as a whole. FNSFs are 2.6 times more common for every reduction of one standard deviation of femoral bone mineral density(13).
As can be seen, many of these risk factors may be rooted in sub-optimum nutrition, and eagle-eyed athletes, coaches and clinicians will recognise how many of these are typical characteristics of eating disorders and relative-energy deficiency syndrome (RED-S – readers are directed to this article for a more in-depth discussion). The take-home message therefore is that knowledge of an athlete’s eating habits can provide an additional and valuable insight as part of a diagnosis, when FNSF is suspected in a female (or indeed male) athlete, and also for athletes to determine if they may be at risk of an FNSF in the future.
Diagnosing FNSF
The presentation of FNSFs in athletes such as runners is often vague and non-specific(14,15). Worryingly perhaps, evidence suggests that around 75% of FNSFs are either misdiagnosed or undiagnosed following a physical examination(16). The typical symptoms in athletes with an FNSF are as follows:
- A gradual onset of groin or hip pain over a period of time, which is increased by activity and/or weight bearing. This may progress, possibly causing a limp during walking.
- Pain that is reduced or even eliminated with non-weight bearing rest.
- Pain that is localized to the front of groin region or thigh, the outer side of the gluteal (buttock) region, or pain which radiates down to the knee.
- Pain that is increased with either greater exercise duration or higher intensity.
- In the early stages of FNSF, pain that manifests towards the end of exercise. However, as the injury worsens, pain that manifests throughout exercise, and eventually is even present during rest and at night.
- In severe cases where a fracture is complete or displaced, athletes may report a popping or cracking sensation during exercise(17,18).
As previously alluded to, where there is a suspicion of FNSF, the athlete’s recent training history needs to be considered carefully. Has there been a significant increase in volume or intensity in recent months? Has the athlete switched training on harder surfaces – eg from trail to tarmac? In addition, the athlete’s nutritional habits should be carefully considered – both current and those in the past. In female athletes, an indication of menstrual history is also very important to consider. More generally, where there is any suspicion of FNSF (ie symptoms described above), athletes and/or their coaches and trainers should immediately seek expert help from a physiotherapist, who in turn should refer the athlete for imaging as soon as possible.
What imaging is best for diagnosis?
While X-ray imaging is a useful first step, its value for diagnosing an FNSF is limited since it has a low sensitivity for early detection of an FNSF (15%) and at only 50% sensitivity at follow-up(19). Therefore, where there is a strong suspicion of FNSF, MRI imaging is the gold standard for obtaining a correct and early diagnosis – essential to prevent an incomplete fracture from becoming complete or even displaced.
It is important to understand that X-ray imaging is not sufficient to properly diagnose a FNSF. Not only does it frequently fail to show any clear findings when an FNSF is present(20), it frequently shows complete FNSFs as incomplete fractures, whereas subsequent imaging using CT or MRI is better able to diagnose the presence and nature of the fracture(21). Of all the imaging modalities, MRI evaluation is the most sensitive and specific for the diagnosis of FNSF as it can detect the early, low-grade and subtle bony changes associated with FNSFs(12). In short, if an athlete or his/her coach suspects the possibility of an FNSF, he/she should insist that MRI imaging and not just X-ray imaging is carried out!
Treatment for FNSF
Although they often involve surgery, the treatment options will depend on imaging findings. In the case of an undisplaced, compression side, incomplete fracture, a 4-week period of conservative (ie non-surgical) management may be initially recommended. This will require the athlete to rest completely and be non-weight bearing, with follow-up imaging to assess bone healing. If progress in healing is observed and no pain is experienced, the patient can gradually introduce partial weight bearing using crutches then very gradually progress onto full weight bearing, with further imaging to assess bone healing. Where diet and vitamin D status are known to be poor, an increased intake of vitamin D and calcium-rich foods is recommended, using supplementation if necessary.
A non-surgical treatment option is of course far more preferable than an athlete having to undergo surgery. This explains the importance of early and accurate diagnosis using an awareness of early symptoms and the right kind (MRI) of imaging. When FNSF symptoms first appear, athletes should most definitely not try and train through them but seek advice. Likewise, they should not be fobbed off with X-ray imaging alone, which is unlikely to reveal an FNSF in its early stages.
In the case of tension-side fractures, and all complete and displaced (ie severe) fractures, surgery is recommended. It is also recommended for athletes who, having attempted conservative treatment, are still experiencing pain after four weeks of rest. Although it is beyond the scope of this article, FNSFs are surgically treated using metal-constructed internal fixation devices. Currently, the best surgical option is considered to be the ‘screw-plate’ fixation as it provides a superior support for hip loading in all three planes of movement(22). In the longer term, athletes with poor nutritional habits should be counselled by a qualified nutritionist as to the importance of nutrition for bone health and minimizing the risk of a future stress fracture.
References
- Belcher A. Ueber den Einfluss des Parademarches auf die Entstehung der Fussgeschwulst. Med Klin 1905; 1: 305-306
- Arch Phys Med Rehabil 1999; 80: 236-38
- Sports Health 2013; 5: 165-174
- J Bone Joint Surg Br. 1961;43:647–663
- Clin Orthop Relat Res. 2018;476(2):441–445
- American Journal of Sports Medicine 16.4(1988): 365-377
- Curr Osteoporos Rep. 2006 Sep; 4(3):103-9
- American J Sports Med 2004; 32(6): 1528-1534
- American J Clin Nutr 1990;51(5): 779-783
- Bennell K., Malcolm SA, Thomas SA, Ebeling PR, McCrory PR, Wark JD, Brukner PD. Risk factors for stress fractures in female track-and-field athletes: a retrospective analysis. 1995
- Sport Med 1999; 28: 91-122
- Acta Biomed 2017; Vol. 88, Supplement 4: 96-106
- Br Med J 1996; 312: 1254-1259
- Acta Orthop Scand 2002; 73(3): 359-68
- Eur J Orthop Surg Traumatol 2012; 22 Suppl. 1: 103-6
- American journal of sports medicine 44.8 (2016): 2122-2129
- Research in Sports Medicine 2016; 24(3): 283-297
- J American Academy of Orthopaedic Surgeons 5.6 (1997): 293-302
- Operative Techniques in Sports Medicine 17.2 (2009): 90-93
- Military medicine 2015; 180(1): e134-e137
- Bone. 2012 Nov;51(5):929-32
- Am J Sports Med 1996; 22: 168-176

Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.