You are viewing 1 of your 1 free articles. For unlimited access take a risk-free trial
Cool it: can cryotherapy work for athletes in the long term?

New research investigates whether repeated sessions of cryotherapy for short-term recovery help or harm long-term training adaptations
As any physiotherapist will tell you, if you want to dampen down the inflammation swelling of an injury, the golden rule is to ice it, ice it early and keep on icing it! The reason is simple; as soon as tissue (ie muscles, ligaments, tendons) is damaged, the body’s healing process sets in – and that involves inflammation. Sometimes this inflammation is all too apparent (for example a twisted ankle that swells up like a balloon), while at other times it’s hidden from view (such as with a shoulder impingement injury, where the inflammation occurs deep in the joint).Inflammation after exercise
Inflammation is the body’s basic response to injury. When an injury occurs, your body immediately recognizes the damaged tissue as ‘foreign’, and a sequence of complicated and interrelated events are set in motion to defend the body and eradicate the damaged tissue by a process of destruction, followed by renewal. It’s a bit like warfare: if you want your body to be healthy, it must be able to mount an inflammatory response!Although inflammation invariably results from an injury, you might be surprised to learn that to a lesser extent, inflammation also plays a role in the process of training adaptation in muscles. When subjected to an unusually high or extended workload, muscle fibres experience a degree of micro-damage in the form of microscopic tears. This process is entire normal and is known as exercise-induced muscle damage, a process which involves an increase in inflammation(1). Most athletes will be very familiar with this phenomenon as significant levels of micro-damage leads to delayed-onset muscle soreness, or DOMS for short.
While a small degree of DOMS is to be expected from time to time, it can not only feel unpleasant, but also impair an athlete’s ability to resume high-quality training. This explains why much research has been conducted into therapeutic approaches to accelerate recovery and reduce that impact of DOMS as soon as possible. In a comprehensive review study carried out last year, researchers analyzed 120 studies on exercise-induced DOMS and concluded that hot/cold water contrast therapy, cryotherapy, phototherapy, vibration, ultrasound, massage, and active exercise all produce beneficial effects in the management of DOMS-related pain(2).
Cold for reducing inflammation
When it comes to reducing DOMS-related inflammation, we should not be surprised to see that cold therapies such as cold water immersion, ice baths and cryotherapy (where muscles are exposed to extremely low temperatures but for briefer periods of time) are not extremely popular but also very effective. After all, if ice is effective for high-inflammation events such as muscle sprains and tears, it’s hardly surprising that it also aids the reduction of normal post-exercise inflammation and muscle soreness. This explains why these cold therapies have become extremely popular among athletes who need to recover rapidly from a bout of hard exercise to ensure they are fresh to perform at a high level as soon as possible – eg, soccer players during a period of fixture congestion.A this point, the obvious question to ask is if ice baths work to speed post-race/match recovery, can they also speed recovery from hard workouts? As Rick Lovett explains in a previous article on ice bath use, this might seem like a tempting proposition. Religious post-workout icing might allow you to do your next hard workout a day or so sooner — something that in turn would allow you to squeeze in an few extra hard training sessions per month. So if for example, icing would let you do two hard workouts every five days, rather than every six days, that faster recovery would theoretically gain you a 20 percent gain in workout efficiency. For serious competitors that’s a very tempting proposition!
The upside of inflammation
Although it sounds sensible, combating inflammation at every opportunity might actually be quite undesirable. That’s because the benefits of training occur during recovery, as the muscle fibers rebuild and ‘remold’ themselves to be stronger for the next bout of exercise. This is why harder than normal workouts induce significant training effects; they produce micro-damage to muscles (and inflammation), inducing repair processes that leaves muscle slightly stronger, more resilient and with greater oxidative capacity than before. Inflammation therefore is an important part of the adaptation.Trying to ameliorate the body’s normal inflammatory responses following a training session can be thought of as an attempt to force the body to recover more quickly than it wants to. However, it’s a fact of biology and physiology that muscle fibers require a certain amount of time for repair and adaptation processes to occur. If natural post-training inflammation is curtailed in order to accelerate recovery, there’s a good theoretical basis to believe that it could inhibit the training adaptations that occur following a training session. Indeed, scientists now acknowledge that post-exercise inflammation is a means through which muscles can repair and regenerate, thereby facilitating training adaptations(3). In plain English, chilling the muscles down after a training session could reduce the benefits generated by that session.
It turns out that there’s some good evidence for the blunting effects of post-exercise icing. A 2006 study by Japanese researchers investigated the effects of routine ice baths during training(4). Twelve college-aged men trained 3 -4 times per week for six weeks on stationary bicycles at moderate intensity while Another 11 participants trained using handgrip exercises to strengthen their forearms. Following each workout, the research subjects stuck one limb in an ice bath at temperatures ranging from 5°C (for the stationary cyclists) to 10°C (for the forearm-strengthening group). The other limb stayed at room temperature, allowing each participant to serve as their own control.
The results showed that following the 6-week training period, the cyclists’ non-ice-bathed legs had gained more strength, more blood circulation, and more endurance than their ice-bathed ones. Meanwhile, in the handgrip participants, the chilled arms gained 11% in strength, while the non-chilled ones had improved by 16 percent. Moreover, the number of hand squeezes the subjects could perform at 30 percent of maximum effort improved 45% in the un-chilled arms, but only 7.5% in the ice-bathed arms (see figure 1). Further research on cyclists supports this notion(5); when compared with traditional low-intensity cool-downs, post-training ice baths produced less muscle growth.
Figure 1: Hand grip strength & endurance with icing/no icing
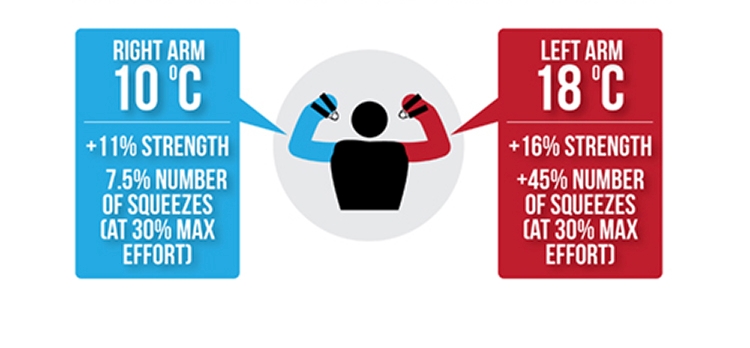
Right arm cooled with icing post training; left arm not cooled.
Despite these findings (of reduced or blunted strength adaptations with regular icing), other studies on the effects of icing and endurance performance have not found such negative effects(6). In fact, when it comes to cold water immersion, research suggests that it actually increases a key signalling molecule known as PGC-1α, which is an established molecular marker in the activation of mitochondrial biogenesis(7). In short, PGC-1α activates genes involved in manufacturing mitochondria – the cells’ ‘energy factories’ – which means they have more capacity to process oxygen and hence (in muscles) have improved endurance capacity. This means that cooling or icing muscles might actually improve endurance adaptations!
Another confusing factor is that nearly all of the research looking at the effective of cold therapy on training adaptations has only investigated training of a single type – namely interval training (for endurance) or resistance training (for strength). However, programmes that incorporate a combination of training methods are arguably much more relevant for athletes, who require a variety of fitness attributes, including speed, power, strength, agility and endurance. Research on the effects of cold therapies when athletes undertake mixed training is scarce. The picture is also confused by the fact that the little research that has been carried out on mixed training adaptations and cooling has been for only short durations – typically around two weeks(8). What’s needed therefore is research investigating the effects of repeated cooling therapy on athletes undergoing mixed (ie normal) training for period of a month or more.
Real life research
The good news is that brand new research by British scientists just published in the journal Frontiers in Sport and Active Living has looked at this question and come up with some answers(9). In this study, the researchers investigated the impact of repetitive ‘whole body cryotherapy’ (WBC - where the whole body is immersed in very cold air for short periods – see this article) on adaptations to a concurrent progressive 6 week training programme involving endurance, strength, and power training.Twenty trained male volunteers were recruited for the study, with 10 randomly assigned to receive WBC and 10 assigned as non-cryotherapy control group (CON). As it turned out, three of the cryotherapy participants withdrew due to injury during their program while one control participants withdrew due to illness – therefore 16 participants completed the study. Before and after the 6-week program, all participants were assessed for body fat levels, VO2max (maximum oxygen uptake capacity), muscle torque, three repetition maximum barbell squat and countermovement jump height. The mixed training program itself consisted of four sessions per week:
- Two 30-minute treadmill runs at 1% incline (initial intensity set at 70% VO2 max).
- Two strength and plyometric training sessions with 2-minute recoveries between sets.
- Barbell squats (4 × 6 repetitions at 70% estimated one repetition maximum)
- Dumbbell lunges (3 × 8 reps on each leg)
- Nordic leg curls (2 × 8 reps)
- Depth jumps (3 × 8 reps from a box height of 30cms)
- Split lunge jumps (3 × 8 reps on each leg with hands on hips)
The WBC participants received cryotherapy treatment within 30 minutes following completion of their first and final training sessions each week. Before entering the chamber, participants wore a head band, face mask, gloves, socks, elbow and knee bands, and clogs. Participants entered the cryotherapy chamber, initially exposed to a vestibule chamber at −60°C for 30 seconds, followed by the main chamber at −120°C for 150 seconds. On completion, the participants were advised to stay mobile before changing back into usual clothing.
What did they find?
The key findings from the study were as follows:- Participants in both groups significantly improved muscle torque, with the gains experienced being similar in both groups (see figure 2).
- Both groups significantly improved their barbell squat performance, with similar gains between the two groups (see figure 3)
- There was no significant increase in VO2max for either group.
- The control group experienced a significant gain in their countermovement jump performance; how the WBC group experienced no such gains (see figure 4).
Figure 2: Muscle torque gains after six weeks
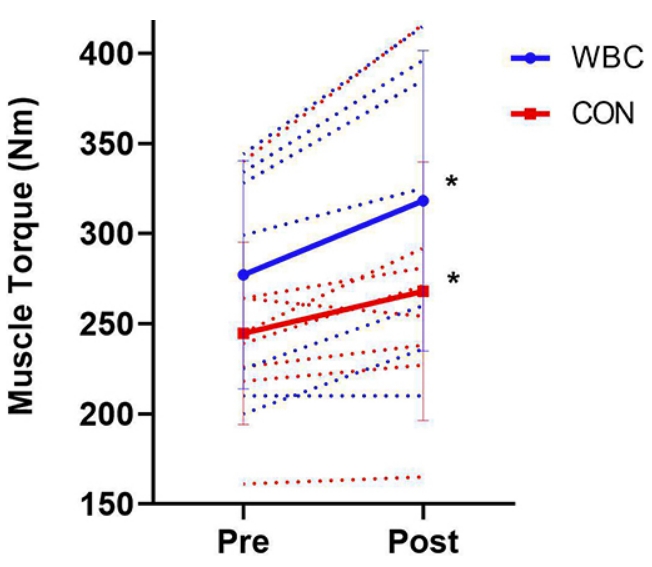
WBC = whole body cryotherapy; CON = control group; each dotted line = individual participant; gains were not significantly different between the groups.
Figure 3: Barbell squat gains after six weeks
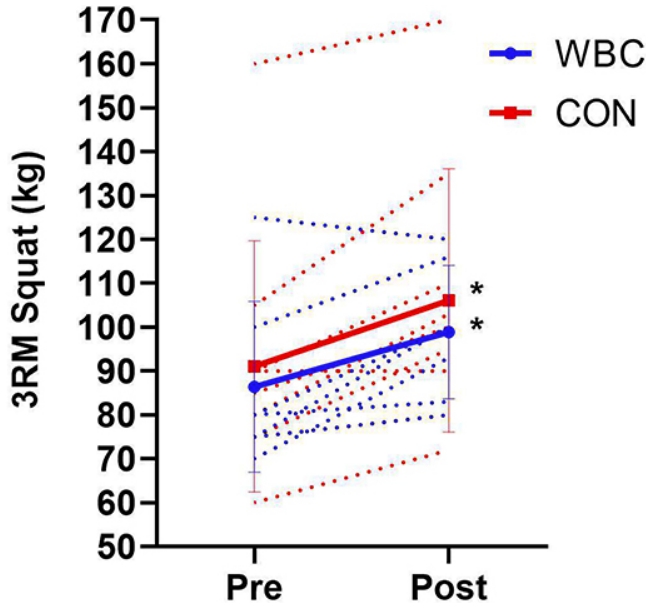
The squat performance gains achieved by both groups were similar.
Figure 4: Countermovement jump performance gains after six weeks
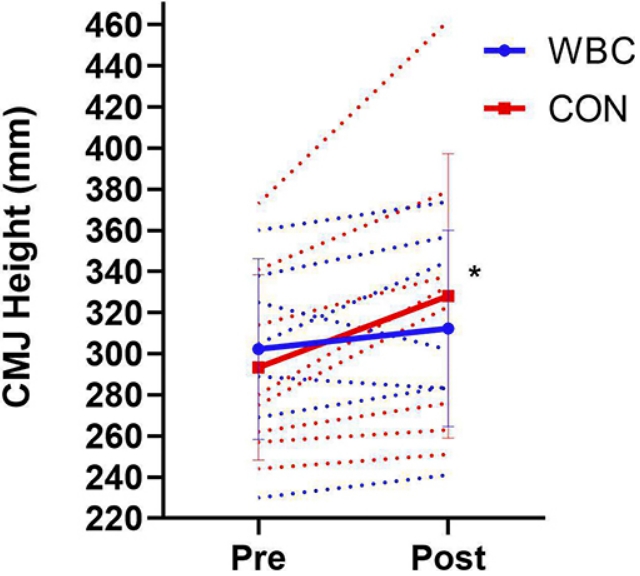
When it came to countermovement jump performance, only the control group improved, suggesting that the WBC therapy may have blunted this particular training adaptation.
Conclusions and implications
This is one of the first studies to investigate the impact of repetitive cold therapy treatment on adaptations to a combined strength and endurance training program. Overall, we can see that the training program was generally effective in improving lower body strength and maximum muscle torque (power) in both groups, regardless of whether cold therapy was used or not. And while there were no significant gains in aerobic endurance, the WBC didn’t appear to have a detrimental impact on these overall fitness attributes.Where it may have had a detrimental effect is on countermovement jumping performance; here the WBC did not achieve any gains over the six weeks, while the control group did. Therefore, it’s quite possible that the WBC therapy may have caused an interference effect in the development of explosive power. However, we will need some more data from larger studies before we can be sure of this effect. Also surprising is that unlike some previous studies highlighted above, the use of WBC did not blunt strength adaptations.
A possible explanation for this is that WBC was used twice per week rather than after every single training session. Also, the earlier studies showing blunted strength adaptations used cold water/ice immersion, which exerts a significant hydrostatic pressure on the muscle – possibly hindering blood and amino acid flow to muscles (essential for growth and recovery). In this study, cryotherapy was conducted using supercooled air for very short periods, which would not exert quite the same effect.
In terms of athlete recommendations, we can say that because WBC did not blunt strength adaptations, but may have a possible negative impact on explosive power development this has implications for the use of cold therapy. It may for example be preferable for athletes to undergo repetitive cold therapy treatments throughout training phases where there is higher priority for general strength development than explosive power – for example, early in the season. When explosive power is the goal, cold therapies might be best shelved. For the competitive or tapering phases of athletic training programming, when athletes are more concerned with exercise recovery as opposed to training adaptations, it seems that cold therapies such as WBC can offer significant recovery gains without any major drawbacks!
References
- J Sports Sci Med. 2021 Oct 1;20(4):655-664
- Phys Ther Sport. 2021 Nov;52:1-12
- Inflamm. Res. 2016; 9, 175–186
- Eur J Appl Physiol (2006) 96: 572–580
- Journal of Physiology 2015. 50 593(18)
- Rep. 2019; 9:12013
- Sci. Sports Exerc. 2014; 46, 1900–1907
- Physiol. 2018; 9:1711
- Front Sports Act Living. 2022 Mar 25;4:834386
Read More


Related Files

Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.