You are viewing 1 of your 1 free articles. For unlimited access take a risk-free trial
Stitch: avoid that pain in the side!

The precise causes of a ‘side stitch’ during exercise remains something of a mystery. But recent research provides a better understanding and also paves the way for solutions
You’ve trained hard, built high levels of fitness and are ready for action. Then out of the blue and without any warning it strikes – the dreaded and disabling pain of stitch that you just can’t seem to shake off. Sounds familiar? Well, don’t worry because you’re in good company. Stitch can affect even the fittest athletes; witness Haile Gebreselassie’s spectacular exit from the 2011 London Marathon all because of a mundane side stitch! Mundane it may be, but a full-on stitch is not only painful, it can also wreck the best-laid exercise plans. So what exactly causes stitch and how can it be prevented?What causes stitch?
It may sound bizarre, but the despite the fact that stitch is such a common phenomenon, it’s actually very poorly understood. One of the main reasons for this is that because it’s unpredictable in its occurrence, stitch is hard to study. In other words, you can’t set up a simple experiment in which you induce stitch in your subjects and then try and observe that physical changes that take place because it’s often not possible to induce a stitch even when you create favorable conditions (eg training on a full stomach). And by the same token, you may find that stitch occurs in subjects who would not be expected to suffer from it! This means that very few properly controlled scientific studies into stitch have actually been carried out.Despite the dearth of scientific data on stitch (more technically known as ‘exercise-related transient abdominal pain or ETAP for short), there are a number of theories about the fundamental causes of stitch. Included as being possible theories are the following(1):
- Stitch is caused by an insufficient flow of blood to the diaphragm, which in turn causes a muscular spasm or ‘cramp’.
- Movement of the stomach and liver during activities such as running places stress on the diaphragm ligaments and/or the ligaments supporting the abdominal organs, causing discomfort
- Stitch is caused by an irritation of the lining of the abdominal cavity, which occurs as a result of friction generated between the (moving) abdominal organs and the relatively static wall of the cavity.
Predisposing factors in stitch
It may be hard to carry out controlled experiments on stitch, but there’s plenty of data out there about the nature and most commonly observed circumstances of stitch. This is gathered by looking at large numbers of cases where stitch occurs and then trying to tease out any common factors – a so-called epidemiological approach. Although it’s not the same as measuring direct cause and effect, it does give scientists a very useful insight into what might lie behind its occurrence. When the data on stitch occurrence is analyzed, certain associations become apparent. These are as follows(3-6):- Stitch is more common when there’s lots of repetitive torso movement; for example a running stitch is twice as likely as a waking stitch and ten times more likely as a cycling stitch.
- The older you are, the less likely you are to suffer stitch, but your gender and (surprisingly) fitness level appear not to be factors in susceptibility. However, the more frequently you train, the lower appears to be the risk of stitch.
- The occurrence of stitch appears to be increased when food or drink is ingested in the two hours or so prior to exercise; fruit juices and carbohydrate drinks seem to increase stitch risk over plain water.
- Most stitch occurs in the mid or lateral abdominal area (see figure 1), although it can sometimes lead to referred pain the right shoulder – indicative of the association of the diaphragm muscles.
- The discomfort associated with stitch is often aggravated by breathing but may be relieved by bending forwards while contracting the abdominal muscles, or tightening a belt around the waist.
Figure 1: Most common locations for stitch sensations
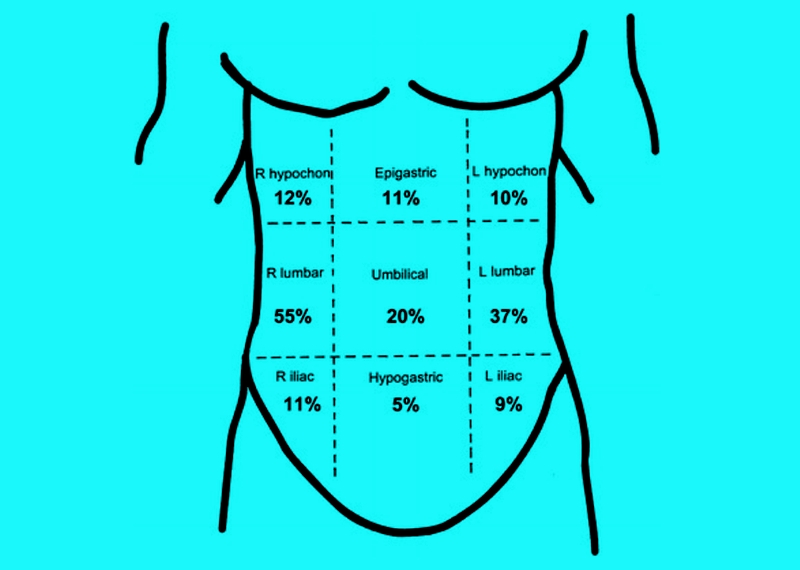
The data shown here for the most common locations of exercise-related transient abdominal pain (ETAP) was derived from 818 symptomatic subjects in two studies by Morton and Callister and Morton et al(7,8). As you can see, the right and left sides are the most common locations. NB: L = left, R = right. Some respondents reported ETAP in more than one position.
Putting the pieces of the jigsaw together from the evidence above, a pattern begins to emerge, which implicates torso movement and the diaphragm in the etiology of stitch. The fact that food or fluid in the stomach increases the prevalence of stitch(9) points to the involvement of organs in close proximity to the diaphragm. Meanwhile, it also occurs frequently in sports that involve jarring and/or twisting of the torso; this provides further evidence that stitch is linked to the movement of the body’s internal organs, and also that factors involved in maintaining postural stability may be important. Some researchers have proposed that an inadequate warm-up prior to exercise and training in cold conditions could help to provoke a stitch(10,11). However, these claims are based on anecdotal observations and cannot therefore be considered reliable. One factor that is more certain however is that stitch’ makes breathing very uncomfortable; it’s hard to escape the conclusion therefore that the pain of stitch and diaphragm function are inextricably linked!
Diaphragm dual role
The diaphragm muscles play a key role in expanding the chest cavity and therefore in the inspiration of air into the lungs. But what is less appreciated is that these muscles are also intimately involved in stabilizing the torso. Research has shown that during the preparatory phase of most limb movements (ie at the point at which movement is initiated), the diaphragm is activated subconsciously(12). In doing so, the diaphragm activation raises the pressure inside the abdomen, which acts to increase spinal stability(13). Therefore, the diaphragm muscles work together with the core stabilizer muscles to encapsulate the abdominal compartment of the body (see figure 2), as well as deep muscles surrounding the spine. This acts to stabilize the spine and pelvis during movements involving the torso such as throwing or lifting.Figure 2: The diaphragm and its relation to core musculature*
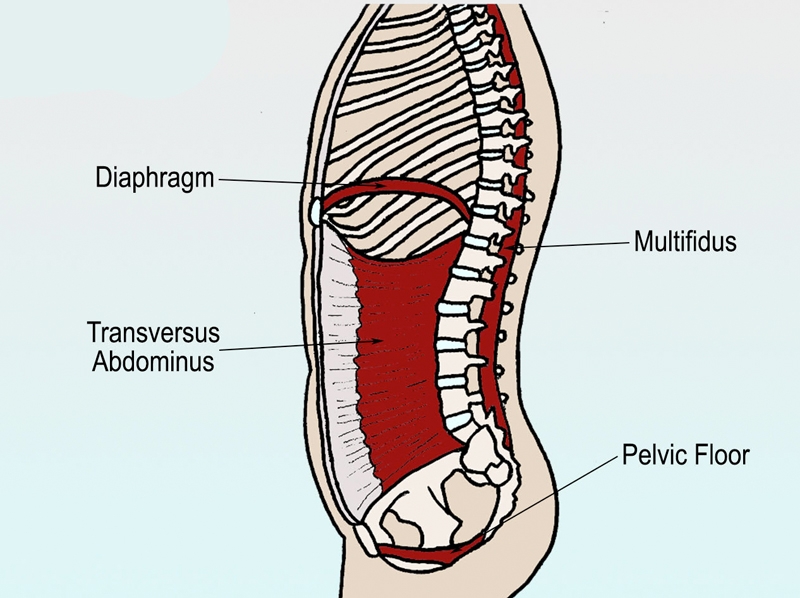
The diaphragm muscles adjoin and work with the deep transversus abdominis muscles of the tummy to provide stabilization of the core. *Image courtesy of ‘Pilates On Fifth’
Given this dual role, it’s possible to see how the diaphragm muscles could become overloaded. Combine the demands of heavy breathing during vigorous exercise with those of stabilizing the torso. Now throw in a bit of organ movement to further interfere with normal diaphragm function, and it very plausible to envisage a scenario where the diaphragm just can’t cope, leading to a stitch(14).
As it turns out, this combination of factors is exactly what happens during running, especially where breathing and stride cadence are difficult to synchronize – for example running cross-country over uneven terrain. In these circumstances, the diaphragm is subjected to buffeting by large organs in close proximity as they move up and down in synchrony with the foot strike. Not only does this stretch the diaphragm, but it also means that the diaphragm then has to work against the buffeting forces, which adds considerably to the amount of work it must do; this almost certainly explains the common observation that stitch and ‘rib ache’ are more common in cross-country runners than road runners.
Overcoming stitch
If the prime cause of stitch is due to the inability of the diaphragm muscles to adequately perform both breathing and core stabilizing functions, can they be trained to become more efficient – ie to reduce the likelihood of a stitch? Given that the diaphragm muscles are trainable like any other muscles, the intuitive answer would seem to be yes, and some evidence does indeed suggest that training and strengthening diaphragm function does lower the incidence of stitch.UK researcher Professor Alison McConnell has been one of the world’s leading authorities in this area, and she and her team achieved some very promising results with the use of diaphragm training devices such as ‘Powerbreathe’ (see this article). These devices place a ‘load’ on the diaphragm during inspiration and used regularly have been shown to improve performance by making exercise feel easier, and by preventing the inspiratory muscles from diverting blood away from the legs during exercise, thus improving endurance performance.
One of the anecdotal observations of the many subjects who trained their inspiratory muscles using such devices during Professor McConnell’s studies is that they no longer experienced ‘stitch’ pain. Moreover, many subjects also reported that if they trained their inspiratory muscles within an hour or so of going for a run, they often then got a ‘stitch’(15). In other words, they went for a run with the diaphragm in a pre-fatigued state, which predisposed them to getting a ‘stitch’. These observations are strongly indicative that ‘stitch’ is a response of the diaphragm to a situation it can no longer cope with and that training the diaphragm can help reduce the incidence of stitch.
Training to reduce the risk of stitch
What can you do to reduce the occurrence of stitch? The evidence suggests that including some regular inspiratory muscle training (IMT) in your training program will increase the strength and endurance of your diaphragm muscles, so reducing the likelihood of a stitch. A typical session of IMT might consist of inhaling (using a Powerbreathe or similar device) for around 30 breaths with the resistance adjusted so that you can only just achieve 30 breaths in a time period of 2-3 minutes. Training this way twice a day for a period of 4-6 weeks will produce real benefits, not just in terms of reducing stitch risk, but also improving endurance performance generally.You can further enhance the ‘stabilization capability’ of the diaphragm by performing your IMT routine while activating your core muscles – eg while balancing on a stability ball or wobble board. The research also suggests that this capability is further enhanced and made more sports specific is the IMT is performed while adopting the typical posture required in your sport. For example, cyclists should IMT train while leaning forward in a seated position.
Don’t forget too, if you’re prone to stitch, remember to avoid ingesting high-carbohydrate fluid and particularly solid food in the 2-3 hours before training. If this seems rather onerous, the good news is that research shows that regular training after ingesting fluid beforehand seems to decrease the risk of stitch. In other words, it seems it’s possible to ‘train the gut’ to cope with fluid (ie not produce a stitch) provided you practice this in training(16).
Finally, if the dreaded stitch does strike, anecdotal evidence suggests that bending forwards, tightening the abdominal muscles (especially transversus abdominis) and pressing inwards and upwards (hard!) on the site of the pain with your palm for 10-15 seconds will help to alleviate the pain. Failing that, you can always slow down or even stop if need be, and if even after following all these recommendations you occasionally have to, don’t be too hard on yourself – after all, stitch can strike even world champions!!
References
- Br J Sports Med 2003 37: 287-8
- Sports Med. 2015 Jan;45(1):23-35
- Med Sci Sports Exerc 2002 34: 745-9
- Med Sci Sports Exerc 2000 32: 432-8
- Med Sci Sports Exerc 1999 31: 1169-75
- Int J Sport Nutr Exerc Metab 2004 14: 197-208
- Med Sci Sports Exerc. 2000 Feb; 32(2):432-8
- J Sci Med Sport. 2005;8(2):152–162
- N Z Med J. 1951 Dec; 50(280):607-12
- N Z Med J. 1986 Jun 25; 99(804):469
- Arch Intern Med. 1941;68:94–101
- J Appl Physiol 89: 967-76, 2000
- J Biomech 38: 1873-80, 2005
- J Physiol 537: 999-1008, 2001
- J Strength Cond Res. 2016 Oct;30(10):2942-51
- Curr Sports Med Rep. 2006 May; 5(3):161-4



Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.