You are viewing 1 of your 1 free articles. For unlimited access take a risk-free trial
Conquering the death zone: lessons for all athletes
What are the challenges of high-altitude climbing, and what training and psychological insights can mere mortals learn from the world’s greatest climbers? Andrew Hamilton explains

At 4,000 feet you get a sense of achievement and some great views. At 15,000 feet, the thrill is magnified by the fitness, technical knowledge and planning required to reach the summit. At 20,000 feet the air is so thin and depleted of oxygen that you need to spend several weeks acclimatizing at altitude in order to avoid debilitating and potentially life-threatening acute mountain sickness (AMS). At 24,000ft (7,300m), you enter another and even more deadly world – the death zone (see figure 1).
Figure 1: Barometric pressure as a function of altitude
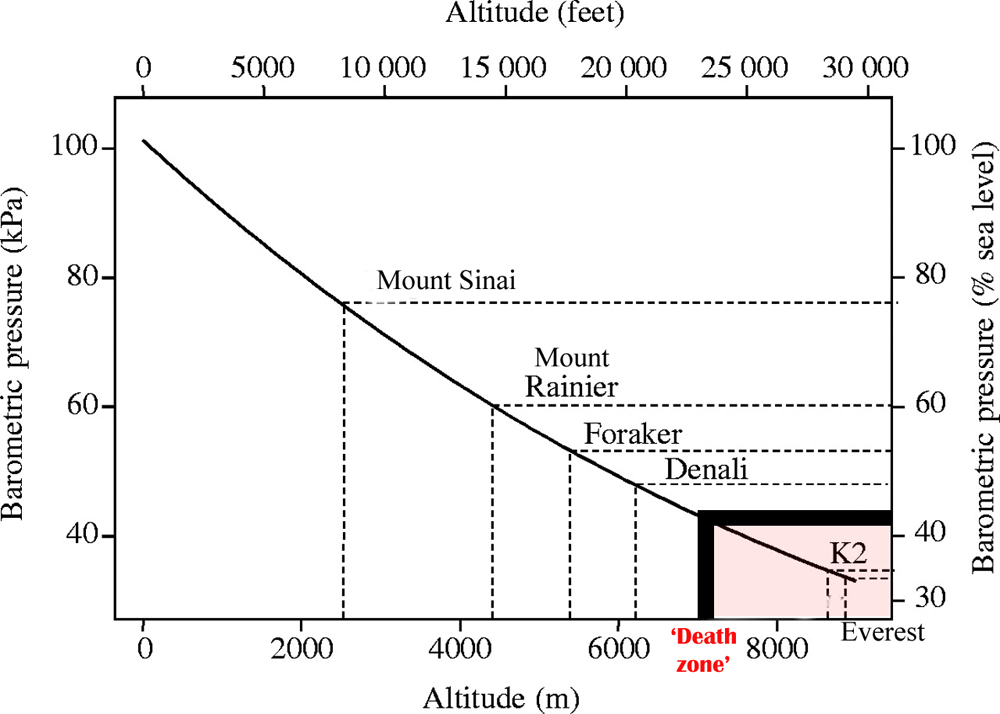
The left-hand axis shows absolute pressure in kPa, while the right-hand axis shows pressure as a percentage of sea-level value. The dashed lines show altitudes and estimated relative barometric pressures of various localities or summits. The red zone represents the altitude at which survival for extended periods becomes impossible – the so-called ‘death zone’.
This death zone is a world where no amount of acclimatization or extra oxygen will stop the brain from swelling or lungs from gradually filling with water. In short, you start to die slowly, and descent to lower altitude is all that can save you. And at these altitudes, a rescue is almost certainly out of the question; even in perfectly benign weather, the world’s most technologically advanced helicopters are virtually unflyable. You really are on your own.
What is acute mountain sickness (AMS)?
As you ascend up to around 1,500m (4,800ft) above sea level, the reduction of oxygen in the (slightly thinner) air is minimal and exercise capacity is not significantly different from sea level(2). But above 1500 metres, the reduction in oxygen starts to make itself felt; exercising feels harder than that performed at the same pace at sea level and both heart rate and breathing rate are increased for a given pace.
Physical and psychological effects of altitude
However, it’s above 3,000m (10,000ft) that the reduced barometric pressure – and therefore partial pressure of oxygen – really begin to make themselves felt. The significant drop in oxygen availability and oxygen saturation levels can produce a range of physiological and psychological disorders, known as Acute Mountain Sickness (AMS). Athletes or climbers who move suddenly to such an altitude or higher can experience symptoms such as breathlessness, headache, insomnia, dizziness and abnormal tiredness, and mood disturbances. In addition, cognitive function can be impaired, resulting in reduced reasoning, memory, concentration neuromuscular control and coordination(3).
Life threatening
At higher altitudes still, AMS can become life threatening due to ‘high altitude pulmonary edema’ (fluid on the lungs) and ‘high altitude cerebral edema’ (fluid on the brain). When this happens, it is essential for climbers/athletes to be moved to lower altitude or sea level as quickly as possible. For any given altitude, AMS symptoms usually peak during the first two days after moving to that altitude. Provided the change in altitude is not too great, symptoms recede rapidly in those who adapt providing they remain at that altitude. However some people fail to adapt, and must be moved to lower altitude. Likewise, symptoms can return in those who adapt but move up to yet higher altitudes too soon.
Once of the difficulties in managing AMS is that the number of symptoms, severity and rapidity of the onset and duration of high altitude symptoms vary between individuals, as does the ability to adapt(4). This means that there is no foolproof way of knowing in advance who will be most vulnerable to AMS, especially in novice climbers and athletes. It also means a ‘gently does it, try it and see’ approach is a must when moving to higher and higher altitudes.
Physiological and psychological insights
Discussing the physical and psychological challenges of high-altitude exercise is all very well, but what does it really involve in terms of human experience? To try and translate theoretical discussion into reality, I sat down and spoke with British climber Alan Hinkes, who is a high-altitude mountaineer from North Yorkshire in Northern England.
Back in May 2005, Hinkes was the first ever British mountaineer to summit all 14 of the 8,000m+ peaks in the world, all of which are in the Himalayas. At the time of completing his feat, only 12 other mountaineers had reached all of these 14 summits – fewer people than had stood on the moon. Nearly 20 years later, and with far more advanced equipment and technology, less than 50 people have achieved this feat, and only 19 without the use of supplemental oxygen.
Through his late teens and time at university, Hinkes progressed up the ‘mountaineering ladder’ by first taking on the Scottish mountains (sub 4,500ft) and then moving on to the higher and more challenging Alpine mountains of continental Europe (sub 16,000ft). Inevitably though, he succumbed to the lure of the ultimate mountaineering challenge – the Himalayas – and quickly realised that to really take on the 14 8,000m peaks (26,500+ft - see table 1), the time commitments involved meant that he would have to abandon his teaching career.
Himalayan climbing: the challenge of time
In the Himalayas, there are really only two windows of opportunity to tackle the big peaks. The first is in May and the second in September/October. At these times, the weather is relatively calm and settled with a minimum of snowfall and storms. By contrast, June, July and August are monsoon months with extremely heavy snowfall and a high avHinkesche risk. Once October has passed and through to early May it’s just too wintry and stormy to contemplate climbing in the region.
To ‘summit’ a Himalayan peak in May, you really need to get to the region in March and make the trek to base camp at about 5,500 metres (18,000-19,000 feet). This allows you to simultaneously build your walking/climbing fitness and to acclimatise to the altitude. All in all, 6-8 weeks should be considered the norm for tackling a ‘big’ peak’, something that’s not always compatible with the demands of a 9-5 job!
The ‘big fourteen’ 8000+m peaks
|
Name |
Location |
Height (metres) |
Date conquered |
1990-2010 death rate(% of attempts) |
Everest |
China/Nepal |
8848 |
1996 |
4.4 |
|
K2 |
China/Pakistan |
8611 |
1995 |
19.7 |
|
Kanchenjunga |
India/Nepal |
8597 |
2005 |
22 |
|
Lhotse |
China/Nepal |
8511 |
1997 |
2 |
|
Makalu |
China/Nepal |
8470 |
1999 |
8.5 |
|
Cho Oyu |
China/Nepal |
8201 |
1990 |
2 |
|
Dhaulagiri |
Nepal |
8164 |
2004 |
11 |
|
Manasulu |
Nepal |
8163 |
1989 |
13.4 |
|
Nanga Parbat |
Kashmir |
8125 |
1998 |
5.5 |
|
Annapurna |
Nepal |
8091 |
2002 |
19.7 |
|
Gasherbrum I |
China/Pakistan |
8064 |
1996 |
8.8 |
|
Broad Peak |
China/Pakistan |
8047 |
1991 |
8.6 |
|
Shisha Pangma |
China/Pakistan |
8046 |
1987 |
0.5 |
|
Gasherbrum II |
China |
8034 |
1996 |
16.8 |
There are 14 peaks in the world above 8,000 metres, all of them in the Himalayan/Karakoram region. These are listed below together with the years that Hinkes successfully climbed them. For perspective, the death rates associated with climbing attempts are also given. Note that the mountain height does not necessarily equate to death risk.

The psychology behind the athlete
What drives someone to abandon a secure career for the pain, uncertainties and dangers of high-altitude mountaineering? According to Hinkes, it’s about the triumph of mind over matter. As he explained, “What I did was the ultimate test. Above 7,000 metres, no one can help you should something go wrong; helicopters can’t hover to pluck you off the mountain and you’d have actually more chance of being brought back from the moon! You can’t live at that altitude for more than five days. Your blood becomes ever more viscous because you’re continually blowing off moisture and if you fall and break a leg, you’ll almost certainly die, not of the broken leg, but by the relentless onset of AMS, which causes you to drown in your own accumulated lung fluids in a couple of days. And that’s of course assuming that the severe cold or an avalanche hasn’t already finished you off. Himalayan climbing is about more than a physical challenge – it’s about pitting yourself against your human fears and weaknesses, knowing that each climb could be your last.”
The hardest challenge
There’s no such thing as an ‘easy’ 8,000m climb, but according to Hinkes, it’s K2 (the second highest mountain in the world) that takes the honour of being one of the very toughest 8,000m climbs of the lot. At 8,611 metres, K2 is almost as high as Everest but far more technically difficult and dangerous.


So many people have died on K2, even in excellent climbing conditions, it has been calculated that without oxygen, once you reach the summit, you have nearly a 1 in 5 chance of death – well over double the death rate that of Everest despite the lower altitude(5). Indeed, in the year Hinkes conquered the summit, he was one of only five climbers who succeeded compared with eight mountaineers who died, and K2 was not conquered again for many years afterwards.
In 1994, Hinkes attempted K2 and got to within just 200 metres of the summit. However, at this altitude, every foot of ascent becomes agonising and tortuously slow. To scale that last 600 feet would have taken him around five and a half hours. But with an exceptionally high avalanche risk, Hinkes decided it wasn’t worth the risk. As he himself put it, ‘no mountain is worth a life’. But to get so close to the summit only to be forced into turning back (ruining a trip lasting five months) proved extremely demoralising.
He finally conquered K2 the following year, which was even more impressive as he had been badly injured in a fall in the Nepalese mountains earlier that year and had had to return to the UK to regain his fitness. This meant the subsequent build up and acclimatisation was rather rushed. However, despite taking nearly 14 hours to cover the final 600 metres from the shoulder of K2 to the summit, Hinkes finally made it. As he described, “I stayed on the summit for nearly an hour, longer than I really should have. At the top it’s not over – you still have the equally dangerous descent. On the way back down, I felt my limbs becoming heavier and heavier and moving felt like wading through thick porridge. K2 is such a hard and dangerous climb. Nothing would get me up there again – ever.”
Oxygen and 8,000m climbing
Many of you reading this will be performing regular aerobic conditioning as part of your training program. But what does it actually feel like to breath air containing just one third of the oxygen found at sea level? And what kind of advantage does using artificial oxygen confer?
According to Hinkes, the sensation of performing physically in the death zone without oxygen is almost impossible to describe. “Climbing at extreme altitude without oxygen feels like agony, even torture. You gasp for air while your head is pounding and your body feels as though it’s being crushed in a vice. Every move you make has to be so slow and deliberate – you almost feel like you’re using a Zimmer frame. Then there are the effects of oxygen deprivation; your thought processes become slowed and the distinction between the reality of your situation and your fantasies becomes increasingly blurred. It’s this effect that leads many altitude climbers into making fatal errors of judgement.”
When it comes to the use of extra oxygen to assist extreme altitude climbs, Hinkes has mixed views. He believes that while many climbers brag about the fact that they have conquered high altitude peaks without oxygen, the reality is rather different. “When a climber doesn’t use oxygen, it’s more than likely because of the cost. To transport pure bottled oxygen out to the Himalayas is expensive – it generally has to come a long way and costs a fortune. Secondly, although oxygen reduces risk by enabling you to think more clearly, the oxygen bottles themselves are heavy, increasing your workload; if a climber carries less water to the summit because he or she is using oxygen, that in itself may be a disadvantage, especially given the critical importance of staying hydrated. To make matters worse, if the valve on the oxygen bottle suddenly freezes up, you’re in big trouble. The sudden drop in oxygen concentration reaching the brain can be fatal.”
Hinkes also points out that high-altitude climbers need to be aware that no amount of oxygen will prevent the onset of AMS if something goes badly wrong above 6,000 metres. Unless you can get yourself back down, the end result is the always same – death. In fact, he only ever once used oxygen in the Himalayas and that was on Everest when a national news broadcasting company who were making a documentary on his exploits paid for it!
Hydration
Poor hydration is known to increase the severity of AMS(6). This complicates matters for high altitude climbers. One of the biggest challenges of all at extreme altitude is to stay hydrated. In the rarefied and dry atmosphere of high altitude, water is rapidly lost from the lungs via ventilation; not only is the air at these altitudes almost devoid of water, increasing the rate of water loss with each breath, the low oxygen content means that ventilation is increased dramatically for even very low amounts of activity, thereby further increasing water losses(7). This in turn makes the blood more viscous, impairing physical performance and mental judgement as well as increasing the risk of conditions such as thrombosis.
As Hinkes explained, “Everything about high-altitude climbing makes staying properly hydrated a massive challenge. Living in a tent on a Himalayan mountain slope is like living under a kitchen table in a freezer. There’s no water and it’s such a hassle to get fluid because you have to make it from snow and ice using a stove for melting. Given the importance of fluid for performance, I’ve often wondered how on earth I survived up there. Everything’s such a huge effort at high altitude. Despite knowing you’re severely dehydrated and at risk, and even when your pee has turned dark orange colour it’s almost as though you can’t be bothered to drink the water you’ve just made. It’s as though your body switches off. And there’s no point in trying to use these tube and bladder drinking devices either; they either freeze up, or become rancid!"
The final challenge: Kangchenjunga
Kangchenjunga is an extremely difficult climb for all sorts of reasons. For starters, it’s very remote and inaccessible, lying in the far east of the Himalayan range. This means a long and gruelling trek into base camp with no easy access to villages for supplies of food. Secondly, as well as being one of the highest, the mountain is physically large, and involves longer stretches of horizontal walking at very high altitude in addition to the ascent. There’s also the ever-present risk of rock falls. Thirdly, the weather in this region tends to be more severe, increasing the risk of high winds and avalanches.
Kangchenjunga was the last of the big 14 peaks left for Hinkes to conquer, which he finally achieved in 2005. It wasn’t meant to be that way though. His first attempt was in 2000, when he made it to within 570m of the summit, but decided to turn back due the snow and extreme avalanche risk conditions prevailing at the time. On the descent, a snow-bridge collapsed and Hinkes fell into a crevasse and heard a metallic crack as he hit the crevasse side. He had broken his arm, and still at 6,800m, realised that he was in a perilous position.
“I knew I was in a dire situation. Mentally however, you have to pull yourself together – there’s no point in lying down and dying. And physically you have to be able to handle the pain as well. Making it down was a huge struggle. The rest of the descent was very scary. I couldn’t use my left arm for abseiling or to hold a pole, and with the very deep snow to wade through it was very hard work. I forced myself to concentrate on getting the technicalities right and do what I do best – climb. If I had paused to contemplate the true danger of my situation, I would have almost certainly been overcome with fear and panic, and died as a result.”
Hinkes returned to Kangchenjunga in 2005, and after a failed attempt on the summit on 29th May due to bad weather, he finally reached the summit on 30th May at 7pm, thus achieving his ambition to become only the thirteenth person ever at that time to conquer the ‘big fourteen’.
Training
How should a high-altitude climber prepare for the rigours of this exceptionally demanding sport? According to Hinkes, although general aerobic conditioning is vital, the most important preparation by a long way is psychological. Dealing with the never-ending cold, the squalor, the suffering and the poor diet that invariably come with the challenge comes as a shock for someone who’s never experienced climbing an 8,000m peak!
Having said that, when back in the UK, he would run for 1-3 hours up to four times per week and included regular off-road mountain biking in his training schedule. Hinkes believes in particular that the muscular demands of cycling and climbing are very similar, and data from the literature on muscle activation and fatigue during climbing lends support to this assertion(8). Moreover, the problems of keeping the extremities warm on the bike in harsh winter conditions provide good mental conditioning! Gym and strength work on the other hand was performed relatively infrequently; for a sports-specific resistance workout, Hinkes suggests loading up a backpack with a heavy load (even rocks!) and doing some steep climb repeats to try and build extra climbing strength.
Facing adversity
Athletes often face adversity – particularly mental adversity – when competing and pushing themselves to the limit. So I therefore concluded by asking Hinkes how he coped with facing the ultimate mental adversity – ie what it felt like to face the real prospect of death on each and every one of his climbs? “To say I didn’t get frightened would be a lie”, he replied. “You do get scared sometimes - very scared. However those are the exact times when you need to think as clearly as possible about your options. Faced with a decision about which way or whether to proceed for your own survival requires a clear head. You have to be able to put your fears firmly to the back of your mind especially as anxiety can waste crucial reserves of energy. You need to focus on the job at hand, focus on doing it well and take it step by step. Often there is only one realistic choice – to press on. If that’s the case you just have to get on with it.” We might not be high-altitude mountaineers, but who can deny these are wise words for all athletes?!
References
1. J. Appl. Physiol. 81, 1850–1854, 1996
2. The physiology of training, Elsevier, 2006. 163-191
3. Simonson ’Acclimatization - High altitude medicine and physiology’ (sixth ed.), CRC Press, Boca Raton, FL (2021), pp. 111-123
4. Sports Med, 1993; 16:97-125
5. J Exp Biol 204, 3115-3119, 2001
6. Wilderness Environ Med. Winter; 17(4):215-20. 2006
7. High Alt Med Biol. 2002 Winter;3(4):361-76
8. Front Physiol. 2018 Nov 27;9:1687

Andrew Hamilton

Latest Issue

Subscribe Today

Newsletter Sign Up
Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today




Newsletter Sign Up

Coaches Testimonials
Dr. Alexandra Fandetti-Robin, Back & Body Chiropractic
Elspeth Cowell MSCh DpodM SRCh HCPC reg
William Hunter, Nuffield Health
Subscribe Today
Latest Issue

Keep up with latest sports science research and apply it to maximize performance
Today you have the chance to join a group of athletes, and sports coaches/trainers who all have something special in common...
They use the latest research to improve performance for themselves and their clients - both athletes and sports teams - with help from global specialists in the fields of sports science, sports medicine and sports psychology.
They do this by reading Sports Performance Bulletin, an easy-to-digest but serious-minded journal dedicated to high performance sports. SPB offers a wealth of information and insight into the latest research, in an easily-accessible and understood format, along with a wealth of practical recommendations.
*includes 3 coaching manuals
Get Inspired
All the latest techniques and approaches
Sports Performance Bulletin helps dedicated endurance athletes improve their performance. Sense-checking the latest sports science research, and sourcing evidence and case studies to support findings, Sports Performance Bulletin turns proven insights into easily digestible practical advice. Supporting athletes, coaches and professionals who wish to ensure their guidance and programmes are kept right up to date and based on credible science.